



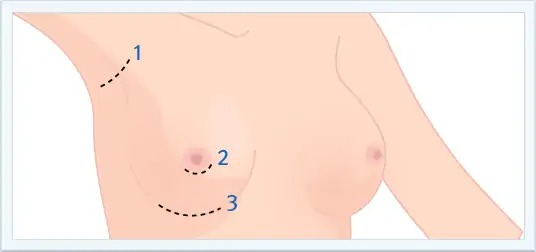
 The approach used in Breast Augmentation is determined by a patient’s individual needs. Before surgery, the type of approach that should be used is determined during consultation. The two that are recommended by Dr. Kim for Asians interested in Breast Augmentation are Inferior breast crease/inframmary fold (IMF) and axillary/transaxillary, but others are listed for consideration.
The approach used in Breast Augmentation is determined by a patient’s individual needs. Before surgery, the type of approach that should be used is determined during consultation. The two that are recommended by Dr. Kim for Asians interested in Breast Augmentation are Inferior breast crease/inframmary fold (IMF) and axillary/transaxillary, but others are listed for consideration.










 From the late 1980s to early 2000, there was controversy regarding the safety of silicone implants in breast augmentation. During this time, silicone implants were used for breast reconstructive purposes without showing any signs of problems. In 1998, a British breast research organization (ING) reported an extensive study and showing that silicone did not cause harm to a person’s body.
From the late 1980s to early 2000, there was controversy regarding the safety of silicone implants in breast augmentation. During this time, silicone implants were used for breast reconstructive purposes without showing any signs of problems. In 1998, a British breast research organization (ING) reported an extensive study and showing that silicone did not cause harm to a person’s body.
 The content of the implant is saline (i.e., salt water), which is inserted into the implant shell via tube during surgery. The shape of the implant may be round or tear-shaped.
The content of the implant is saline (i.e., salt water), which is inserted into the implant shell via tube during surgery. The shape of the implant may be round or tear-shaped.
Records of long-term usage exist, and if the implant ruptures, the implant will change shape rapidly and can be easily noticed – allowing the patient to respond. Additionally, if the implant ruptures or leaks, the saline is easily absorbed without harming the body. However, saline implants are not recommended for thin patients because of implant palpability (i.e., easily seen or felt). Furthermore, subtle waves may be seen by the implant when viewed from the side profile, and there is a loss in volume over time.
 The content of the implant is silicone gel. The shape can be either round or tear-shaped. Older silicone gels consisted of a more liquid substance, but newer silicone gels are firmer and more cohesive. If the shell of the implant does rupture, the probability of the silicone gel leaking to nearby tissue is extremely low. Furthermore, the silicone gel now stays within the scar tissue that normally forms around the implant; therefore, the silicone generally will not make contact with a person’s breast tissue. The feel of silicone gel implants is softer than saline, and unlike saline implants loss of volume does not occur with time. However, if the implant ruptures, the silicone may migrate outside the implant shell. Additionally, if rupture does occur, it may be possible not to notice a change. Therefore, periodic yearly breast exams are recommended.
The content of the implant is silicone gel. The shape can be either round or tear-shaped. Older silicone gels consisted of a more liquid substance, but newer silicone gels are firmer and more cohesive. If the shell of the implant does rupture, the probability of the silicone gel leaking to nearby tissue is extremely low. Furthermore, the silicone gel now stays within the scar tissue that normally forms around the implant; therefore, the silicone generally will not make contact with a person’s breast tissue. The feel of silicone gel implants is softer than saline, and unlike saline implants loss of volume does not occur with time. However, if the implant ruptures, the silicone may migrate outside the implant shell. Additionally, if rupture does occur, it may be possible not to notice a change. Therefore, periodic yearly breast exams are recommended.
 Aesthetic And Reconstructive Surgery of the Breast
Aesthetic And Reconstructive Surgery of the Breast
Saunders Elsevier

The Use of a Retromammary Adipofascial Flap in Breast Augmentation for Patients with Thin Soft Tissue
Aesth Plast Surg
21 May 2018 / Accepted: 14 August 2018
The application of a retromammary adipofascial flap is an effective method of producing natural breast shape and providing additional soft tissue to the caudal breast region.
 Transareolar-Perinipple (Areolar Omega) Zigzag Incision for Augmentation Mammaplasty
Transareolar-Perinipple (Areolar Omega) Zigzag Incision for Augmentation Mammaplasty
Plastic and Reconstructive Surgery, Vol. 135, No. 3
March 2015
The transareolar-perinipple (areolar omega) zigzag incision resulted in satisfactory postoperative scarring and surgical results in Asian patients. This method increases the opening of the areolar incision and can be performed in patients with small (<3.5 cm) areolas. This approach can be an alternative in patients who are prone to hypertrophic scarring.







